
Volume 13 Issues 5 May, 2023

Postgraduate psychiatry training always remains a topic of discussion among academicians and educationalists. In due course of the transition from mental hospitals (better known as Institutes of Mental Health) to general hospitals and the establishment of general hospital psychiatry units (GHPUs), psychiatry training adopted various models and structures to cater to patient care and training in psychiatry (1). Before going further, let you know that the discussion is based on my experience and understanding, and opinions may differ.
We find several combinations and permutations of strategies of organisation results in inconsistency and non-uniformity, which is a big barrier in researching to evaluate the efficacy and suitability of one model over the other. We find two prominent forms of training: a unit system with interunit clinical rotation and a non-unit system with time-based clinical rotation. Here we focus our discussion on a non-unit system with time-based clinical rotation compared to a typical unit system in GHPUs.
A unit system with interunit clinical rotation: is usually followed in an annual system, where admissions and final exams of postgraduates occur annually. Most state or private medical colleges under the National Medical Commission’s (NMC) control fall into this category. Here a certain number of faculty members are grouped to constitute a unit as per their levels of seniority. The Units are allotted specific days of outpatient and inpatient services to provide care to the patients and to be followed up longitudinally by the same unit. The case is usually admitted under the name of the head of the unit, the senior faculty in the unit, and the clinical care shared by all unit consultants. The trainee (senior and junior residents) undergoes a clinical rotation around the vertical organisation of these hierarchical units. This organisation is suitable for larger GHPUs with adequate resources and manpower to divide them into units justifiably.
A non-unit with time-based clinical rotation: This model differed fundamentally from the traditional unit system in combining a flat faculty organisation and a time-based clinical rotation. We can divide the discussion into a non-unit or a flat organisation and a time-based clinical rotation (TBCR).
a. A non-unit organisation: in contrast to the unit system, it is more common in institutions with a semester system, biannual admissions, and final exit exams of postgraduate trainees take place and beyond the purview of NMC, such as Institutes of National Importance (INIs) with a GHPUs fall in this category. Here the department is divided into various sections based on types of service like OPD, IPD, community psychiatry, psychotherapy etc., like a unit system. Still, the resources and manpower are strategically distributed based on the requirement and utilisation. For example, outpatient services must be strengthened in GHPUs due to limited inpatient capacity, more numbers of residents (based on time-based rotation) and staff can be deployed to that area; unlike unit system, where resources are divided among units, unequal distribution can directly affect the patient satisfaction, waiting time etc.
In a non-unit system, faculty members are not grouped in the units; instead, individual consultants are given outpatient days; the patients are admitted under the individual consultant, who is considered as the treating consultant of that case; the treating consultant is fully entrusted with clinical autonomy for the patient care and their longitudinal follow-up unlike unit system where case admitted under unit head and clinical responsibility shared by other consultants of that unit. In a non-unit system, the hierarchical position remains for administrative purposes or high-stake departmental decisions, for routine clinical care, and academic and research activities; the hierarchy rather flattened to make it more functional; hence, each faculty entrusted with administrative and academic responsibilities as per their choice, interest, and work. For faculty, non-unit or flat organisation has certain advantages, such as better equal opportunities, freedom to use departmental resources, a better sense of autonomy, responsibilities and accountability fostering self-development, and administrative and leadership qualities. Unlike a unit system where resources, trainees and faculty distribution are often unequal, biased, and based on hierarchical status, hoarding resources can compromise the performance of an individual faculty and patient safety (2).
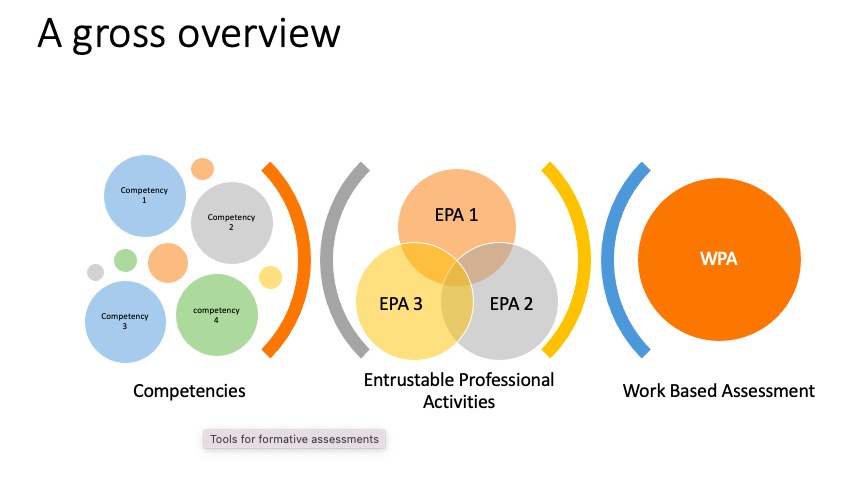
b. Time-based clinical rotation: The trainees, junior and senior residents, undergo a time-based clinical rotation instead of an interunit rotation. Each clinical area has specific learning objectives (SLOs), roles, and responsibilities previously defined at the individual level; the rotation is arranged in an increasing level of difficulties, responsibilities, and competencies. This arrangement is suitable for a fair and robust formative trainee assessment, entrustable professional activities (EPAs) and work-based assessments (WBA) of trainees, which are quite cumbersome to carry out in complex convoluted hierarchical representation (3).
The time-based clinical rotation has a certain advantage over traditional interunit rotation. It is more structured, requires fewer numbers of supervisors, and provides a proportionate variety of clinical and training experience; the student goes through gradually increasing levels of difficulties, fosters time management skills, minimises haphazard instructions, multitasking, dealing with multiple consultants at a time, so-called a hidden curriculum of a unit or hierarchical system, the student’s interests, and performance can be better appreciated, and the learning outcomes are better controlled. Unlike a more faculty-centric unit system, we can consider a flat system with time-based clinical rotation that is more student-centric and training.
We knew from sheer knowledge of management books and organisation strategies that the flattening of hierarchy increases productivity and better utilisation of resources; the hierarchical organisation is preferred for its operational ease due to the centralisation of decision-making(2). A flat system brings individual faculty on the front to confront routine challenges and administrative hurdles, harnessing best of their potential (3), while a unit system provides cosy corners for some to hide, pushing their work down the hierarchy and instrumentalising the motivation and enthusiasm of junior faculties. Unit systems curtail interpersonal issues, perhaps due to imposed silence through complex hierarchical representations, but it also comes with a cost.
Lastly, the flat system with time-based clinical rotation remains a viable alternative; people trained in such a system gradually replicated it in the newly developed AIIMS; hence it is very pertinent to understand it and evaluate the system’s efficacy in the future.
- Chadda RK, Sood M. General hospital psychiatry in India: History, scope, and future. Indian J Psychiatry. 2018 Feb;60(Suppl 2):S258-S263. doi: 10.4103/psychiatry.IndianJPsychiatry_435_17. PMID: 29527058; PMCID: PMC5836348.
- Salehi PP, Jacobs D, Suhail-Sindhu T, Judson BL, Azizzadeh B, Lee YH. Consequences of Medical Hierarchy on Medical Students, Residents, and Medical Education in Otolaryngology. Otolaryngol Neck Surg [Internet]. 2020 Nov 2;163(5):906–14. Available from:
http://journals.sagepub.com/doi/10.1177/0194599820926105 - Allen M, Gawad N, Park L, Raîche I. The Educational Role of Autonomy in Medical Training: A Scoping Review. J Surg Res [Internet]. 2019 Aug;240:1–16. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0022480419301003
This is indeed an innovative idea. The chief advantages are that everyone has to pitch in and do their share of work and also that the degree of training in each individual posting is far superior to that of a unit system. Which should benefit both the trainees and the supervisors in the long run.
Thanks Dr Savitha
Interesting thought. There is a range of complexities of departments and teaching centres, different models May suit different needs. This is a template that can be used in many places. And AIIMS enables innovation to try new means and methods. Commendable
From the point of view of the students, time based clinical rotation ensures equal opportunities among them and from the point of view of teachers it ensures that all students shoulder their share of the workload and in turn minimises chance of resentment among them against each other.Further, it helps in more fexible work distribution among teachers; one can take over the the work of a colleague on leave.
From the point of view of the students, time based clinical rotation ensures equal opportunities among them and from the point of view of teachers it ensures that all students shoulder their share of the workload and in turn minimises chance of resentment among them against each other.Further, it helps in more fexible work distribution among teachers; one can take over the the work of a colleague on leave.
Great beat ! I would like to apprentice while you amend your web site, how could i subscribe for a blog site? The account helped me a acceptable deal. I had been a little bit acquainted of this your broadcast provided bright clear concept
Good web site! I truly love how it is easy on my eyes and the data are well written. I am wondering how I could be notified whenever a new post has been made. I’ve subscribed to your RSS which must do the trick! Have a nice day!
Lovely blog! I am loving it!! Will come back again. I am taking your feeds also.
Thanks for discussing your ideas. I’d personally also like to say that video games have been actually evolving. Modern tools and improvements have served create practical and fun games. These kinds of entertainment games were not actually sensible when the actual concept was first being used. Just like other forms of technology, video games also have had to advance as a result of many years. This is testimony for the fast progression of video games.